
Health care providers are in an acute financial situation. Record-high wages required to attract and retain talent coupled with price inflation not seen since the early 1980s are driving higher costs, while reimbursement and federal policies limit providers’ ability to cover expenses. Adding to this budgetary stranglehold are payment delays and insurance claim denials by payers, which compromise patients’ access to health care and providers’ financial viability.
Several of my colleagues and I had been hearing from some of our company’s members that reimbursement delays and denials were becoming increasingly problematic. We were hearing from chief financial officers, in particular, that this issue was keeping them up at night.
To bring some evidence to the situation, Premier, the company I lead, conducted a voluntary national survey of member hospitals and health systems from mid-October 2023 through the end of December. Respondents were asked to consider all claims from January 1, 2022 to December 31, 2022. The findings are presented as averages, weighted by acute bed capacity of the respondent.
We received responses from 516 hospitals across 36 states, ranging from a 12-bed critical access hospital to large, multi-state health systems.
Straining provider financials
Overall, nearly 15% of all claims submitted to payers for reimbursement were initially denied. Medicare Advantage and Medicaid managed care plans denied claims at higher-than-average rates of 15.7% and 16.7%, respectively.
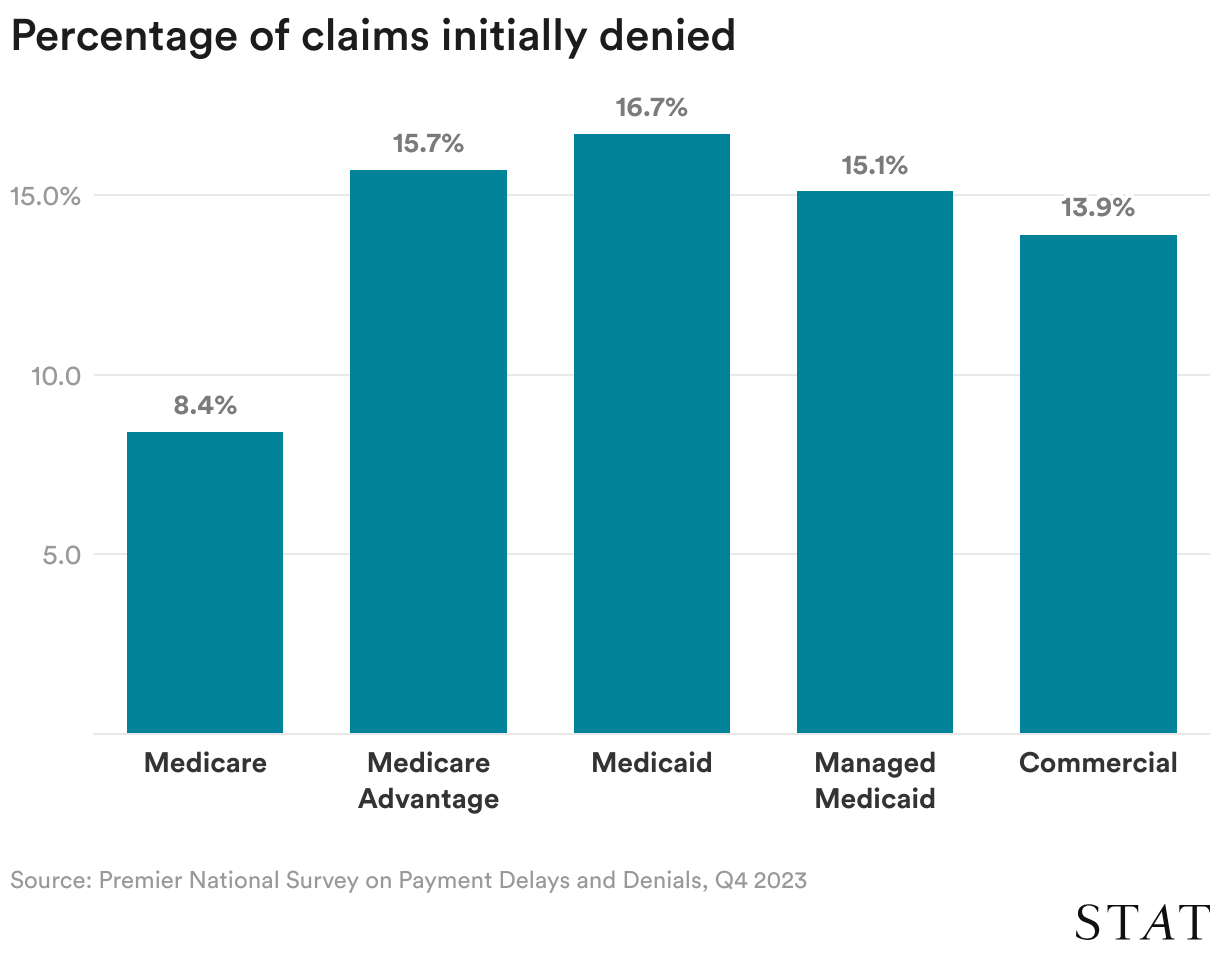
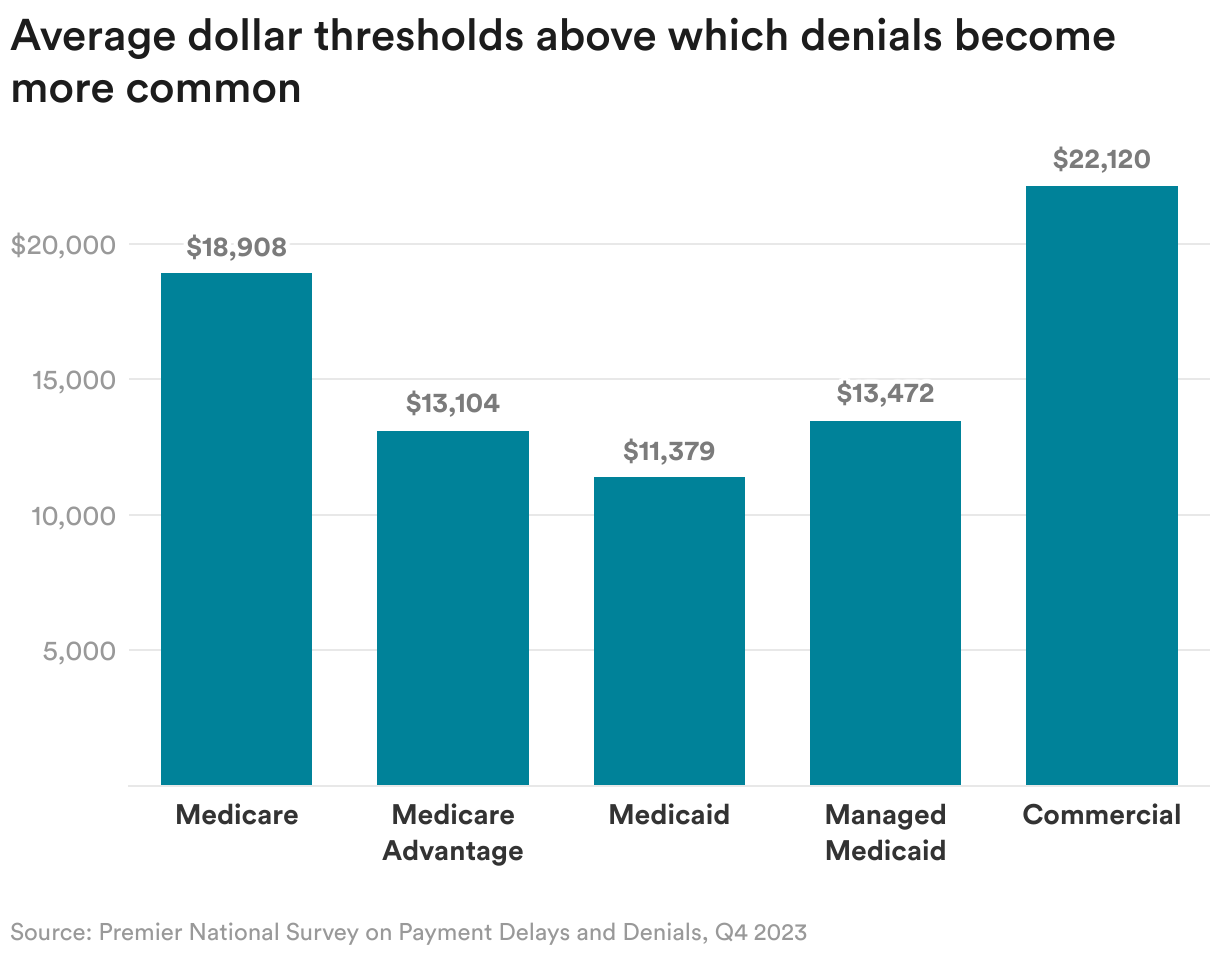
These denials include services that had been preapproved via the prior authorization process, and were more common for treatments costing above $14,000.
More than half of denied claims (51.7%) were eventually overturned and paid. Private payers overturned denials at a higher rate (54.3%) than Medicare and Medicaid (47.9%). But the process of denial and ultimate approval comes with a cost: hospitals and health systems that fought denials did so at an average cost of $47.77 per Medicare Advantage claim and $43.84 per claim across all private payers.
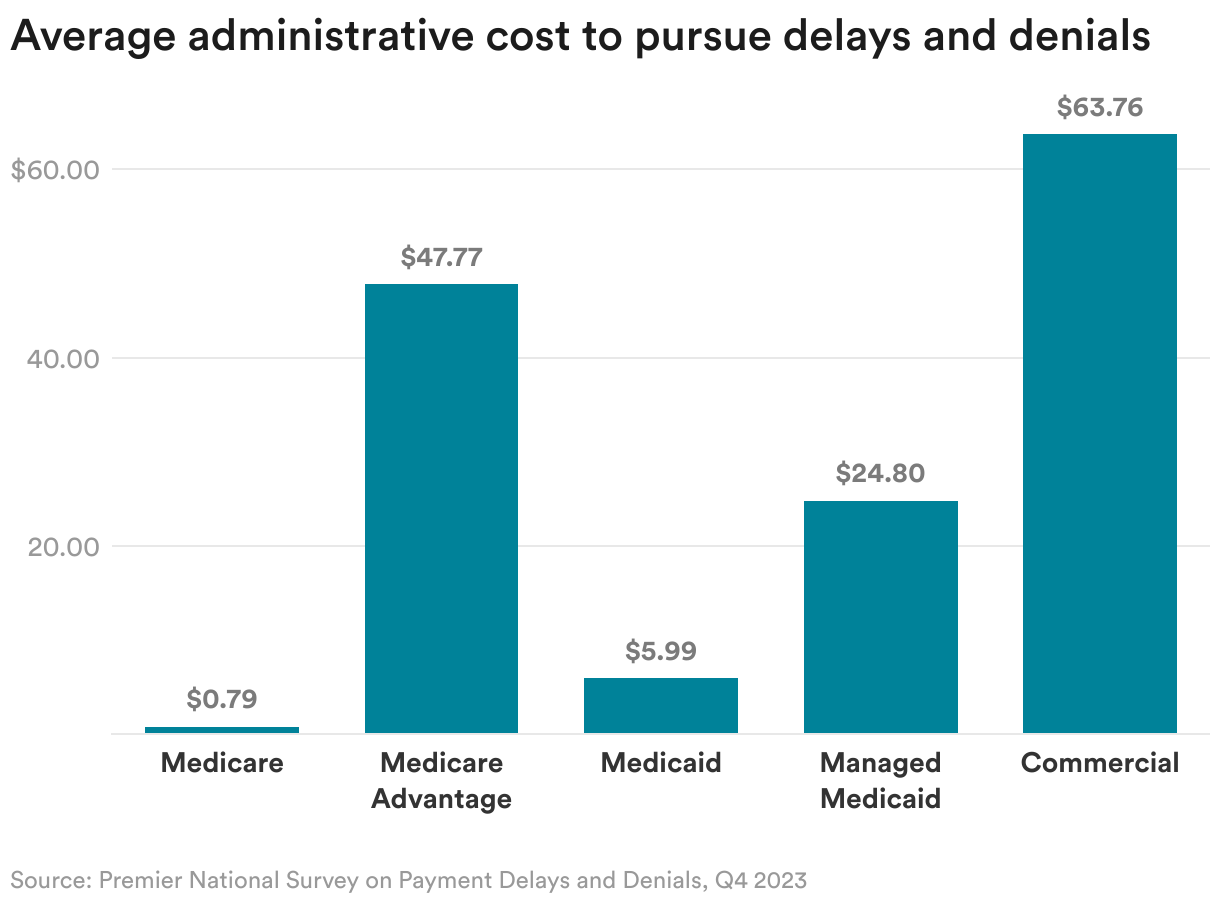
Health insurers process roughly 3 billion medical claims each year. If the rate of denials identified in our survey remains constant over time, that means providers spend about $19.7 billion a year on claims reviews, more than half of which ($10.6 billion) is wasted arguing over claims that should have been paid from the start.
A 2022 U.S. Department of Health and Human study found that, among the payment requests denied by Medicare Advantage plans, 18% met Medicare coverage rules and Medicare Advantage billing rules. Most of these payment denials were caused by human error during manual claims processing reviews (such as the reviewer overlooking a document) and system processing errors (such as a plan’s system not being programmed or correctly updated).
Costly implications for patients
When health plans deny coverage for care, patients may be liable for some or all of the costs, and a lengthy wait for coverage approval may result in patients’ delaying care. Nearly 50% of Americans report skipping or delaying follow-up care because of costs, and the same percentage say they would be unable to pay for an unexpected $1,000 medical bill within 30 days.
Hospital discharges to post-acute care settings such as skilled nursing facilities have faced a disproportionately high level of coverage denials, particularly from Medicare Advantage plans. More than 20% of Medicare Advantage claims requesting discharge to a skilled nursing facility were initially denied.
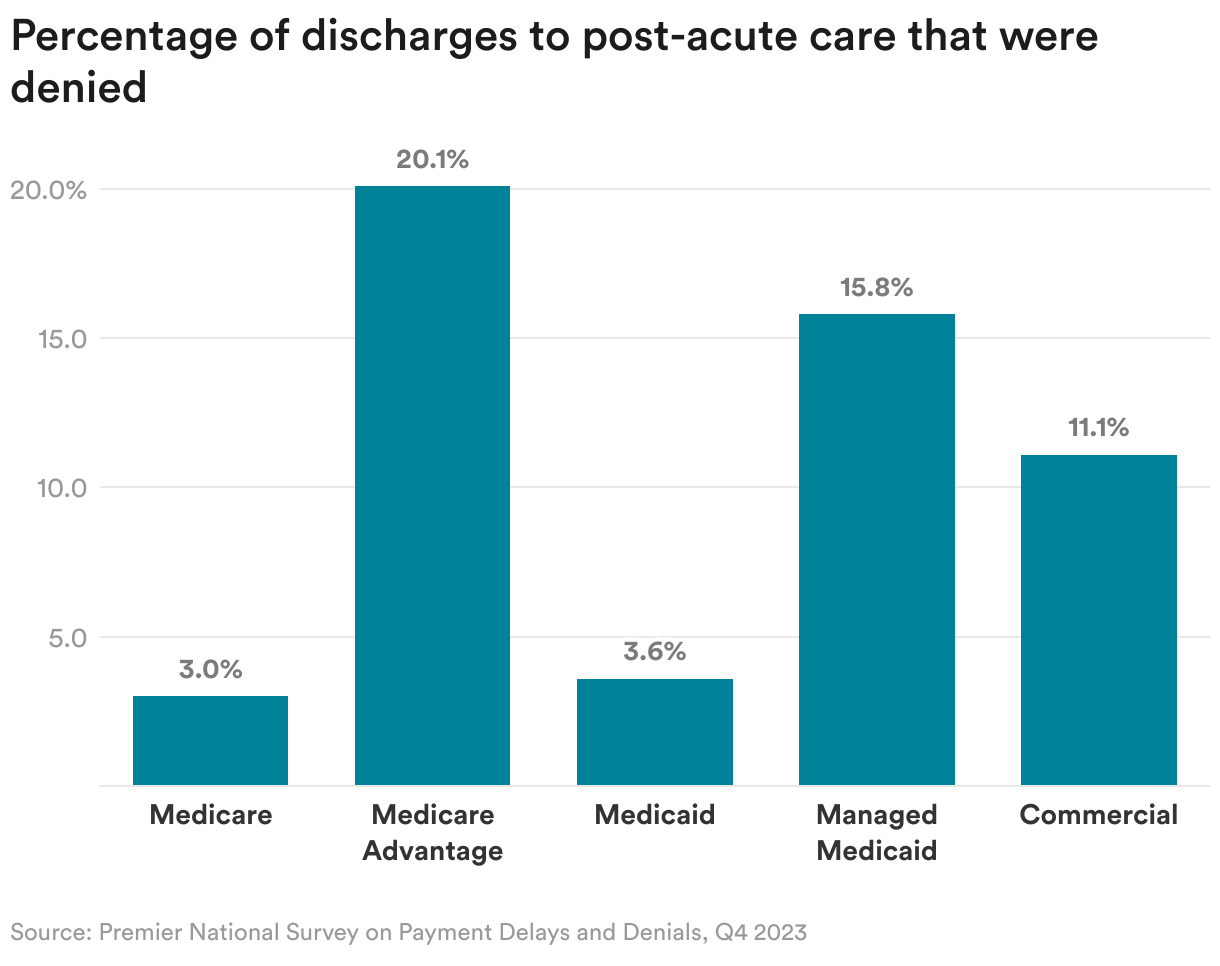
The net result of these denials is longer-than-expected hospital stays, which adds expense and risk, as hospital stays cost more than those in skilled nursing facilities and patients with longer stays have greater rates of secondary infections, falls, and exposure to contagious diseases. Payer denials also have downstream effects on the availability of care, as patients requiring a hospital admission may not have access to a bed until other patients are discharged.
Impacts on hospital quality ratings and reimbursement
Patients facing coverage denials rate their satisfaction with their clinical care 8.2 points lower than patients who do not experience denials. Considering the 15% denial rate, providers’ quality scores may be artificially depressed by payer behaviors.
Poor quality scores have a host of financial impacts for providers. For providers participating in value-based payment models, lower quality scores may curb their ability to earn payment incentives or shared savings — and may even lead to payment penalties.
Providers’ quality metrics are also leveraged by private payers for rate setting, with the highest payment rates reserved for the highest performers. Under the current framework, payers may have incentive to increase denials as that ultimately leads to poorer provider quality scores, which payers may use to reduce reimbursement.
Recommended policy solutions
With its higher-than-average coverage denials, the Medicare Advantage program is a key area of concern — and a vehicle through which the Centers for Medicare & Medicaid Services (CMS) has the statutory authority to immediately act.
Policy levers that CMS could use to address rampant, unnecessary denials by Medicare Advantage plans include:
- CMS should monitor Medicare Advantage plans’ reporting of direct patient care expenditures. It is imperative CMS ensure that the medical loss ratio requirements for Medicare premium dollars used for patient care are in alignment with the benefits to which Medicare beneficiaries are entitled.
- CMS should collect data on payment delays and denials between Medicare Advantage plans and providers to determine whether current practices violate CMS’s expectations around minimum network standards and that beneficiaries have access to the full range of covered services to which they are entitled. While Medicare Advantage plans may claim to contract with providers on paper, actually paying contracted amounts for covered services is critical to continued access to care for Medicare beneficiaries. CMS also must enforce action against Medicare Advantage plans that fail to abide by Medicare coverage rules, which include coverage of post-acute skilled nursing facilities.
- CMS has moved away from holding Medicare Advantage plans accountable for patient experience measures in rulemaking by reducing the weighting of patient experience and access measures in the Star Ratings program. CMS should return to its past policy of weighting patient experience and access measures more heavily in the Medicare Advantage Star Ratings methodology, empowering beneficiaries to hold their health plans accountable.
- CMS should stipulate that claims approved under an electronic prior authorization may not be artificially delayed or denied. Electronic prior authorization should serve as an agreement between the payer and provider to perform the service and remit timely payment for it. Federal regulators should leverage technology to streamline prior authorization as soon as possible.
Refusing or delaying legitimate medical claims has a significant impact on providers and patients. Problematic payer practices strain hospital resources, deplete cash reserves and hinder medically necessary care. The time to act is now.
Michael J. Alkire is the president and CEO of Premier, Inc., a technology-driven health care improvement company.
To submit a correction request, please visit our Contact Us page.












STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect